Chronic diseases such as heart disease, cancer, and diabetes are the leading causes of death, disability, and health care spending in the United States. Many chronic conditions can be prevented, delayed, or caught and treated early. However, despite the progress in research and clinical care, many Americans continue to receive less than recommended preventive health care; this is especially the case for communities that experience a high burden of disparities in chronic diseases. This means not everyone has an equal opportunity to be as healthy as possible.
In 2019, we organized the P2P Workshop: Achieving Health Equity in Preventive Services to assess the state of the science on equity in the use of clinical preventive services and develop a research agenda for moving the field forward.
After the workshop, we brought together representatives from eight NIH Institutes and Offices and seven federal agencies for a Federal Partners Meeting to discuss agency activities and resources relevant to the workshop and create an action plan. Participants identified opportunities for federal agencies to address many of the workshop panel’s recommendations (PDF), organized around four cross-cutting themes:
- Integration of Services and New Delivery Models
- Need for Innovative Methods
- Community Engagement and Systems Approaches
- Workforce and Training.
As we progress through that action plan, we’ve come to recognize that increasing the use of implementation science in the work done by the NIH, our federal partners, and researchers in the field will be a critical part of making progress toward health equity in preventive services.
Why focus on implementation science to improve health equity?
Applying implementation science concepts and methodologies has proven successful in increasing the adoption of many evidence-based practices. Implementation science identifies factors that make it harder or easier to achieve the uptake of evidence-based clinical innovations. We believe that linking health equity research with implementation science offers new possibilities for addressing the workshop panel’s recommendations and improving the use of evidence-based clinical preventive services.
What research is the NIH currently supporting in this area?
To better understand the ways in which implementation science is already being used to advance health equity research—and where it is still lacking—we conducted a brief review of the NIH’s research grant portfolio (PDF) using the NIH RePORTER database.
The review yielded 221 grants awarded from October 2016 through August 2020 that were deemed directly relevant to the workshop’s 10 preventive services of interest, addressed at least one of the four cross-cutting themes identified by our federal partners, and incorporated one or more principles of implementation science (PDF).
Most grants addressed the panel report’s cross-cutting theme 1: Integration of Services and New Delivery Models (82%), while they were least likely to include a focus on theme 4: Workforce and Training (3%). The remaining two themes, theme 2: Need for Innovative Methods (41%) and theme 3: Community Engagement and Systems Approaches (47%), were addressed by just under one-half of the overall number of grants related to the preventive services of interest. Projects testing and assessing multiple preventive services (26%) showed similar patterns across the four cross-cutting themes.
NIH Implementation Science Research Projects Addressing 10 U.S. Preventive Services Task Force-Recommended Preventive Services, by Workshop Cross-Cutting Theme
(n=221 unique grants; 2016–2020)
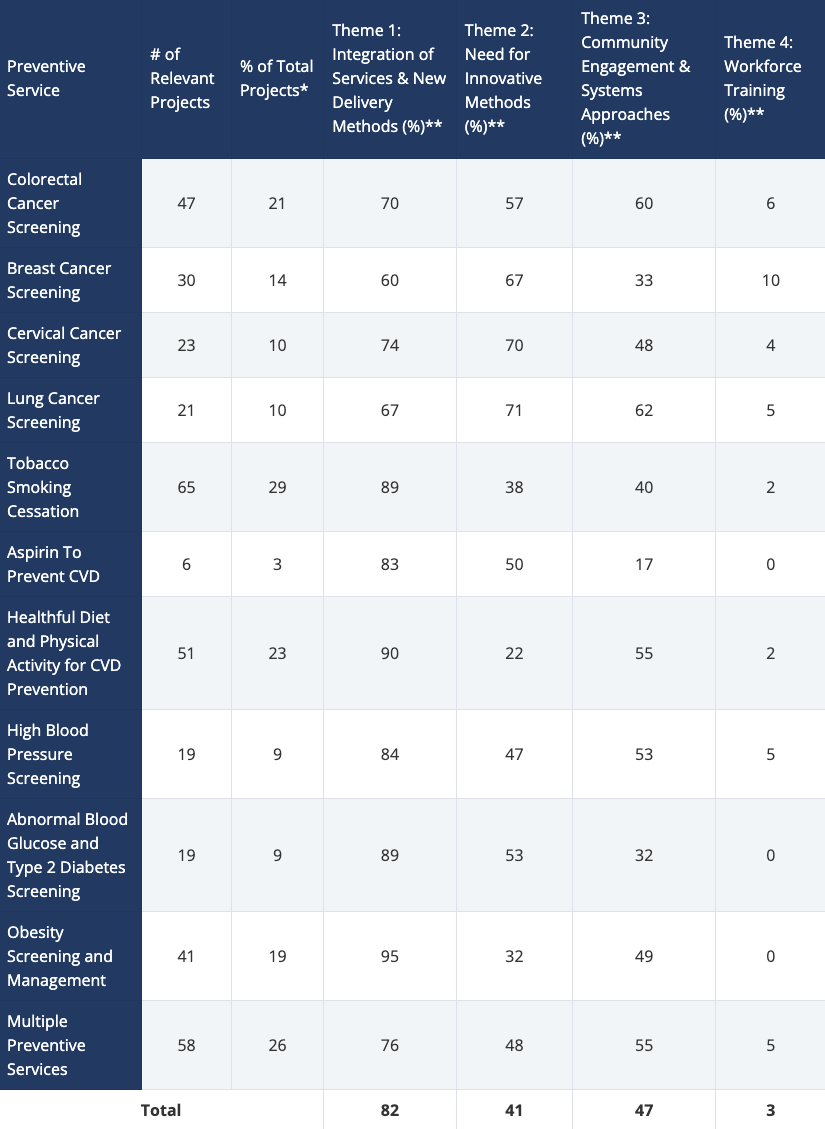
*Grants were mapped onto one or more preventive service(s).
**Total percentages across each preventive service and among total number of unique grants will add up to more than 100% as grants may have been related to one or more workshop recommendation theme(s).
Row totals may exceed the number of relevant grants per preventive service because some grants may have been relevant to more than one recommendation theme.
What more needs to be done?
Invest in Workforce and Training: Our federal partners identified workforce development to increase capacity and competency in health equity as a fundamental investment opportunity. Yet, as noted above, the Workforce and Training theme was addressed by the fewest grants in the NIH portfolio review. We believe barriers to achieving health equity in preventive services will persist without increased and dedicated funding to support interdisciplinary training and career development for the next generation of researchers.
It is also important to determine which elements of diversity and inclusion training are the most effective and may have the most impact in reducing health care providers’ biases. The Institute for Implementation Science Scholars, a program recently funded by the NIH that focuses on applying dissemination and implementation methods and strategies to reduce the burden of chronic disease and address health inequities, may offer important lessons for the field.
Integrate Implementation Science and Health Equity Fields: There is no shortage of research or funding opportunities to improve health equity in preventive services using implementation science concepts, including advancing the science of engagement and outreach to diverse populations, and incorporating social determinants of health (SDOH) and cross-sectoral collaborative models.
Implementation science-focused funding opportunities supported by the NIH, such as the Disparities Elimination through Coordinated Interventions to Prevent and Control Heart and Lung Disease Risk (DECIPHeR) initiative, are ripe for promoting and improving population health in vulnerable, at-risk communities. Moreover, the value of developing new health equity-focused initiatives such as the Implementation Science Centers in Cancer Control Program, the annual Consortium for Cancer Implementation Science working meeting, and the Centers for Diabetes Translation Research program, was reinforced by the workshop’s panel. These initiatives are excellent examples of integrating the implementation science and health equity fields.
Research and implementation science strategies that focus on removing barriers and strengthening the use of clinical preventive services in the context of SDOH offer a more holistic approach to care and have the potential to address multiple levels of influence (for example, factors at the individual, interpersonal, and community levels). Implementation science and health equity experts should also collaborate from the very beginning to reach consensus and embed relevant approaches into research activities early on, which will help speed the translation of effective approaches into clinics and communities of practice.
Research that builds and sustains partnerships across providers, health care systems, and among public and private organizations may offer new avenues for generating evidence on what works in achieving health equity. Ultimately, making health equity a core principle in implementation science research and addressing equity gaps in existing frameworks could contribute to reduced disparities in clinical preventive services.